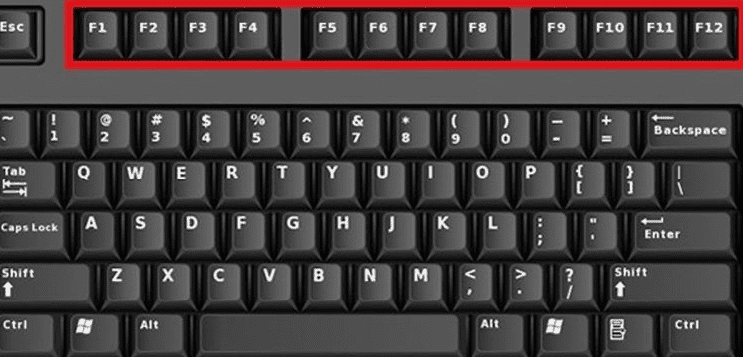
Dacă nu ai folosit niciodată aceste taste pentru că nu știai care este scopul lor, este timpul să dezlegi acest mister. Aceste taste efectuează mai multe acțiuni atunci când sunt utilizate în cadrul sistemelor de operare și a browserelor, deci pregătește-te pentru un curs de bază în tastele funcționale.
Cu lista de mai jos, vei fi înzestrat cu un set de comenzi rapide și soluții ușoare.
F1
Activează imediat meniul de ajutor.
Într-un meniu Windows, când este apăsată tasta Windows, va apărea meniul de asistență și suport Microsoft.
Ctrl + F1 ascunde și afișează meniul în Microsoft Excel și Word.
F2
Îți permite să editezi un folder sau un nume de fișier selectat în Windows Explorer.
În Microsoft Office, apăsând Alt + Ctrl + F2 se deschide Biblioteca de documente.
F3
Îți permite să căuți fișiere în Window Explorer.
Deschide funcția Căutare în browserele web, cum ar fi Mozilla Firefox, Google Chrome
Shift + F3 este folosit pentru a schimba literele în MS Word, inclusiv toate literele în litere mici sau majuscule.
F4
Duplică acțiunea ta în cadrul unui program, cum ar fi desenarea unei linii.
Alt + F4 închide rapid ferestrele programelor active.
În Windows Explorer, plasează cursorul în bara de adrese.
F5
Actualizează paginile browserului de Internet sau ecranul din Windows.
Deschide “Găsiți și înlocuiți” în Microsoft Office.
Începe prezentarea de diapozitive PowerPoint.
F6
Mută cursorul în bara de adrese din browserele web.
Pentru Microsoft Word, deschide următorul panou într-un ecran separat.
Ctrl + F6 îți permite să te miști între mai multe documente Word.
F7
Shift + F7 solicită funcția Tezaur să se deschidă în Microsoft Word.
Alt + F7 verifică ortografia și gramatica în documentele MS Word.
Ai nevoie de traducerea unor documente? Trimite o întrebare echipei noastre de experți lingviști – info@babylonconsult.ro
F8
Lansează modul sigur când Windows se configurează.
În MS Excel, permite Extend Mode pentru tastele săgeți.
F9
Actualizează câmpurile din Microsoft Word.
Ctrl + F9 introduce câmpuri goale în Word.
F10
Deschide bara de meniu.
Shift + F10 funcționează ca un clic dreapta.
Ctrl + F10 maximizează o fereastră în MS Word.
F11
Intră și iese din modul ecran complet în browserele web.
Shift + F11 adaugă o nouă foaie de calcul în MS Excel.
F12
Deschide comanda “Salvează ca” în MS Word.
Shift + F12 salvează documentul în Word.
Ctrl + F12 deschide un document în Word.